|
|
本文经原作者授权进行转载
原帖地址: https://zhuanlan.zhihu.com/p/413306752
之前在备考过程中发现不少关于女性月经周期的题目解释均存在语焉不详的问题,后来查了查相关资料之后发现目前学界对于月经周期背后相关的生理实质仍存在争论。在翻看了FA、Kaplan和几本教材外加查阅了一些文献之后,我从以下两张图中总结了一个可以解释月经周期中激素变化和反馈调节变化的模型,经过和其他小伙伴们讨论之后发现这个模型目前从逻辑上可以较为完美的解释相关的变化,并且对于做题有一定帮助,所以在此将其分享出来,希望能够帮到考U的同仁们。
鄙陋浅见,如若有谬误之处,敬请诸君斧正。
PS:原稿为英文,会在文末附上;本篇文章中文部分如若有欠缺通顺之处,还请诸君海涵。
添加图片注释,不超过 140 字(可选)
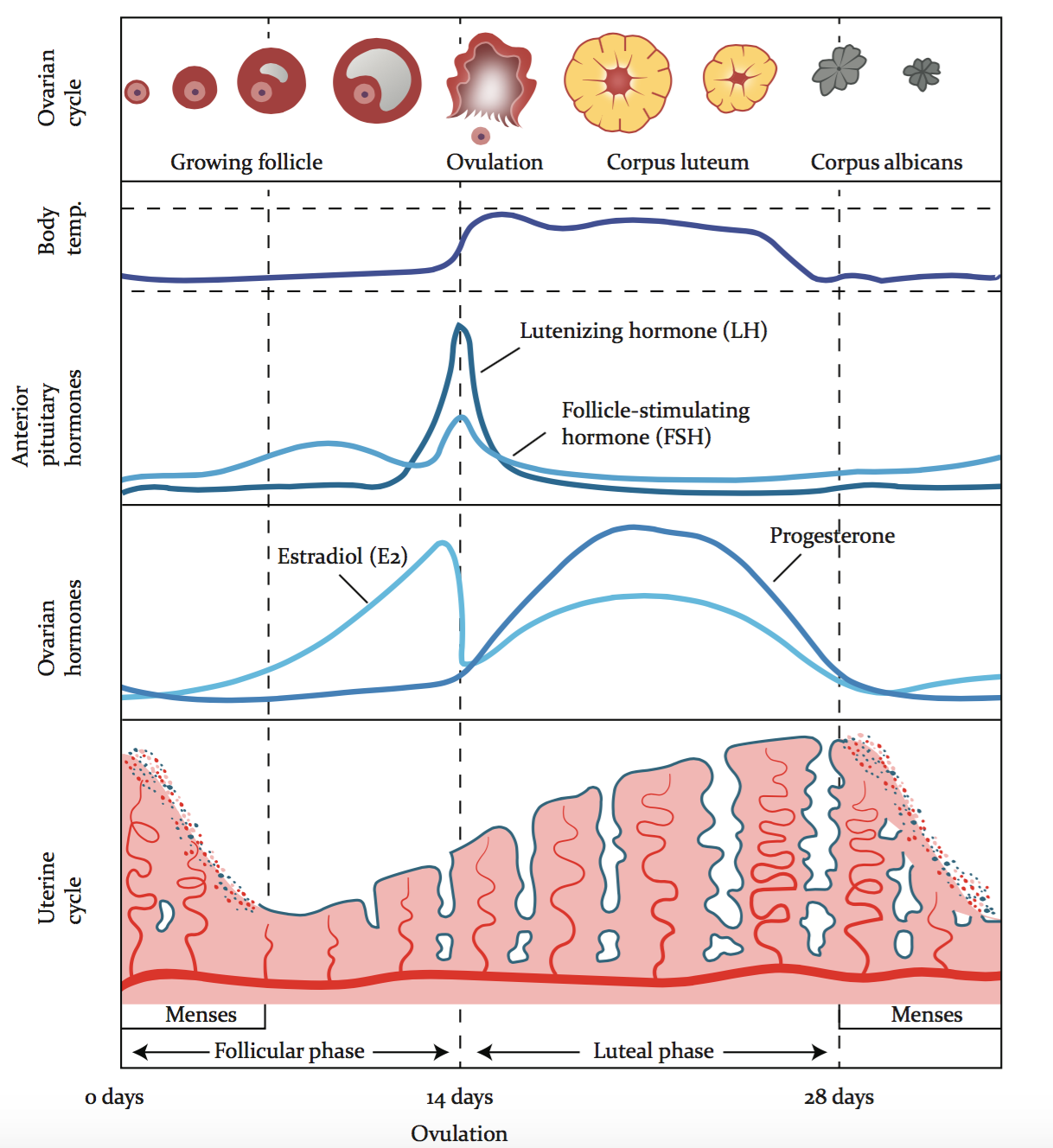
月经周期中的关键事件
典型的月经周期有四个关键事件:卵泡期、排卵期、黄体期和经期。
女性机体的激素水平、卵泡发育程度和子宫内膜状态在这些事件中均会发生对应的变化。
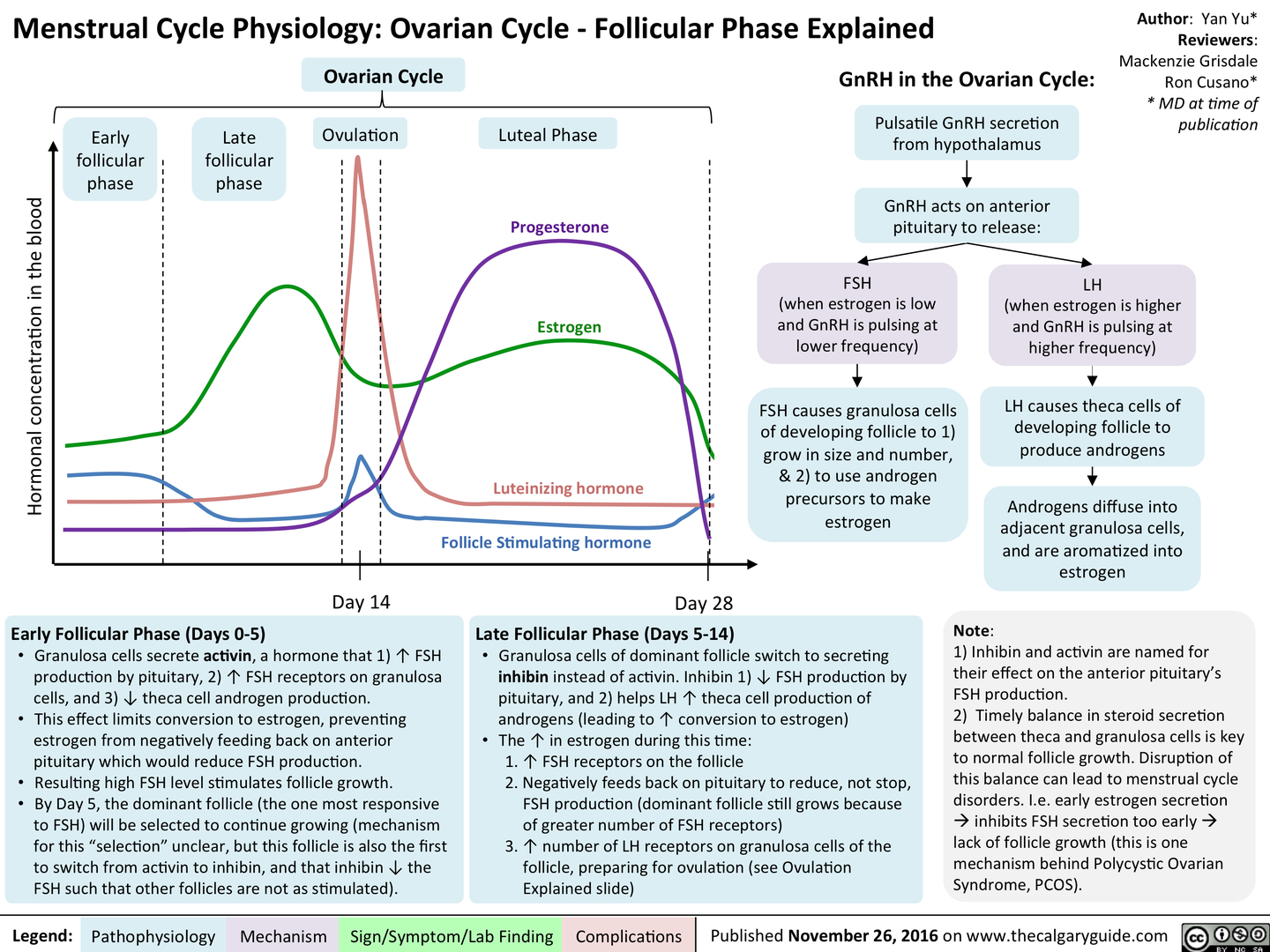
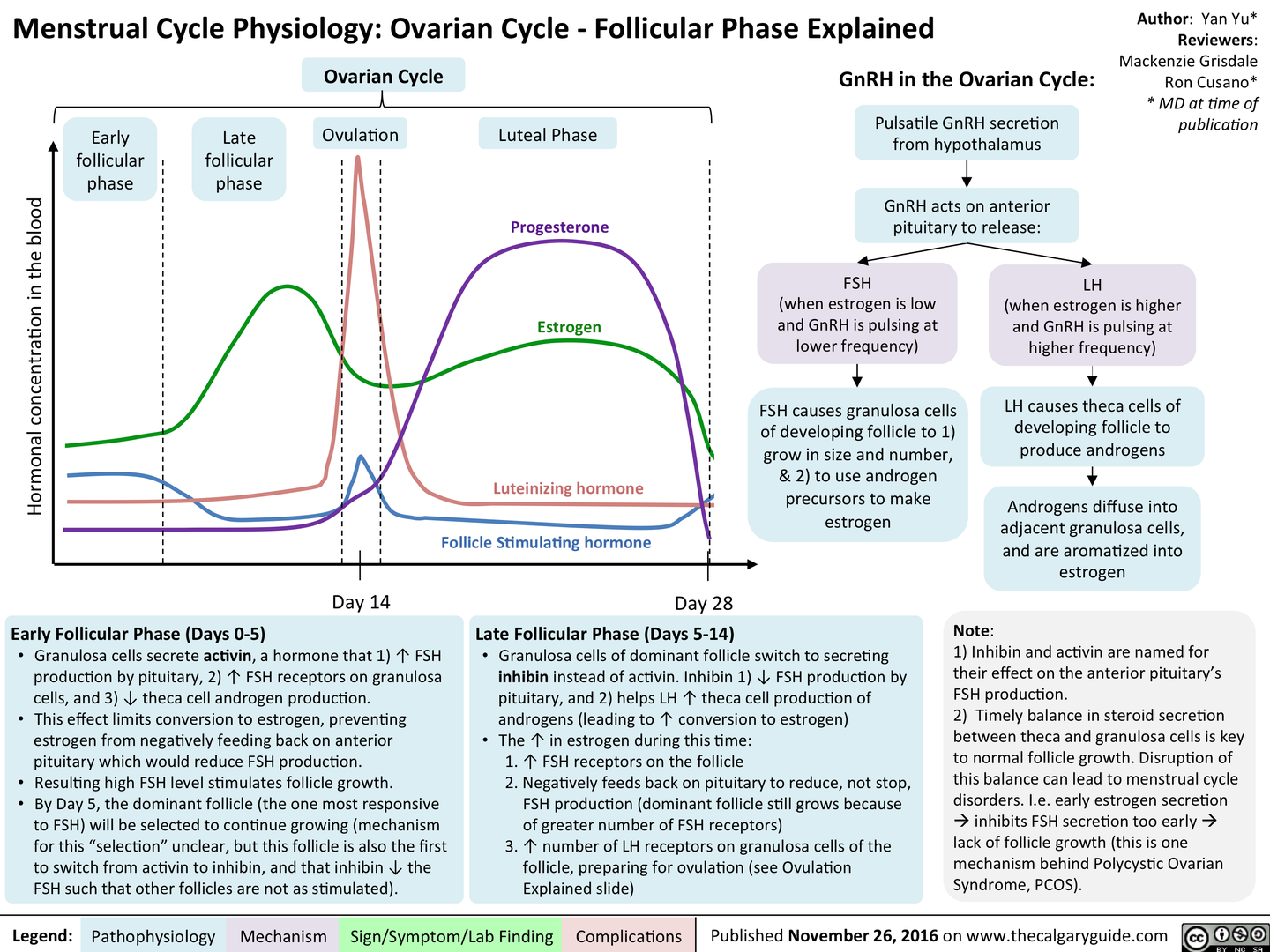
1. 卵泡期
- 促卵泡激素 (FSH) 由垂体前叶分泌并刺激卵巢卵泡的生长
- 优势卵泡产生雌激素,抑制FSH分泌(负反馈),防止其他卵泡生长
- 雌激素作用于子宫,刺激子宫内膜层增厚
2. 排卵期
- 在月经周期中段(第12天左右),雌激素刺激垂体前叶分泌激素(正反馈)
- 雌激素介导的正反馈导致黄体生成素 (LH) 分泌激增,FSH而分泌的增加量相对较少
- LH导致优势卵泡破裂并释放卵子(次级卵母细胞)—— 即排卵行为
3. 黄体期
- 破裂的卵泡发育成缓慢退化的黄体
- 黄体分泌高水平的孕酮,雌激素水平降低
- 雌激素和黄体酮作用于子宫,使子宫内膜增厚(为怀孕做准备)
- 雌激素和黄体酮还抑制 FSH 和 LH 的分泌,防止其他卵泡发育
4. 月经
- 如果发生受精,发育中的胚胎将植入子宫内膜并释放激素以维持黄体
- 如果未受精,黄体最终会退化(约 2 周后形成白色体)
- 当黄体退化时,雌、孕激素水平下降,子宫内膜无法维持
- 子宫内膜层脱落并作为经血排出体外
- 由于雌激素和黄体酮水平现在太低而无法抑制垂体前叶,这个周期现在可以重新开始
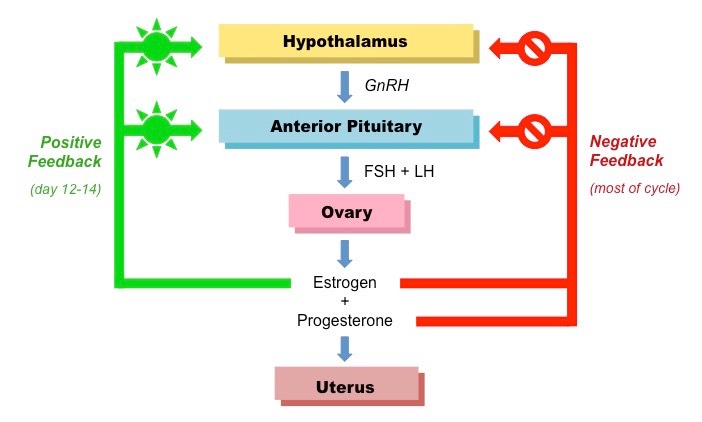
雌激素通过下丘脑-垂体-卵巢轴的负反馈抑制在卵泡期抑制 FSH 和 LH 的分泌。
一旦血浆雌激素水平达到临界阈值,并且该水平保持至少 2 天(成熟卵泡破裂前的时期),负反馈回路将变为正反馈反馈回路和 FSH 和 LH 分泌激增。
------以上为基础知识铺垫------
为了阐释周期内的激素变化,我们可以做一个假设--即卵泡的生长是自发的,不受基线水平血清 FSH 和 LH 水平的调节。关于基线水平对应的具体卵泡周期,等下会为大家详细阐明。
以排卵为线,卵巢中与月经周期相关的结构可细分为两组和三种类型:
只有当一个卵泡达到成熟期时(卵泡期后期),这个卵泡才能产生足够的雌激素,从而达到对GnRH产生正反馈的水平。
由于血清中雌激素水平高,排卵后卵巢内没有黄体,血清中孕激素水平低;因此FSH的升高并不显著(雌激素对FSH本身分泌具有抑制作用),并且由于GnRh升高而刺激LH的分泌。这种波动介导了成熟卵泡在排卵前成为黄体的准备。
此处FSH和LH的峰值源于雌激素对于下丘脑GnRH分泌的刺激作用,FSH本身受到高水平雌激素负反馈调节抑制,因而即使在高水平GnRH作用下水平相对LH仍处于较低水平。雌激素对下丘脑的正向调节作用和雌激素对FSH的负反馈调节作用两者独立存在,并且各自产生对应作用。
排卵后,由于没有成熟的卵泡,下丘脑GnRH的分泌不再受到高水平雌激素刺激,而LH和FSH的峰值在逐渐减少前介导了黄体的成熟。
此后,不断增长的黄体开始分泌雌激素与孕激素,并对 FSH 和 LH 产生负反馈。
在没有受精刺激的情况下,黄体萎缩为白色体,导致 FSH 和 LH 水平不受调节。由于新卵泡在月经后的头几天还在生长,未达到成熟期的卵泡对GnRH没有新的刺激,因此在老黄体萎缩(白色体)和新卵泡生长期间,FSH和LH水平保持正常。
截止此处,我们可以做出如下推论
若以卵泡期前期卵泡未成熟时血浆水平FSH和LH为基线,此时FSH和LH对于未成熟卵泡产生正常催化作用,直到成熟卵泡开始产生大量雌激素并达到阈值以达成下丘脑的正向调节,从而刺激下丘脑大量分泌GnRH,进而导致FSH和LH分泌水平上升,并在排卵前后达到峰值。成熟卵泡破裂后,破裂的卵泡不再能够产生雌激素,故血浆水平雌激素大量下降,导致对下丘脑的刺激消失,且成熟的黄体分泌了阈值以下的雌激素和大量的孕激素,导致FSH和LH从峰值逐渐下降到低于基线水平(此处存疑,白体期前FSH和LH水平具体是否近似于基线水平还待考证)。白体期开始后,在activin和inhibin的综合作用下,FSH和LH水平开始逐渐上升并达到基线水平,及到卵泡期前期时,开始下一个激素调节的循环。
(此处亦可对应开始对于卵泡成长周期本身具有相对自主性的假设:即在卵泡成熟期刺激下丘脑的不一定就是高水平的雌激素,有可能就是成熟卵泡本身或者是位于其内的卵子;破裂的成熟卵泡不具备对下丘脑的抑制功能,而后黄体和白体由于结构的变化亦不能对下丘脑产生直接作用。故而以此推断,雌激素对于下丘脑本身的作用或许也存在唯一性,虽然这一推论本身需要临床科研结果的支持,不过鉴于目前对于月经周期内激素变化的争论学界并未达成统一,本文中所述观点在具体结论出现前亦可作为一种合理的解释。)
"在月经周期中,平均血清激活素 A 水平以双相方式变化(通过方差分析,P = 0.02)
(最高水平在月经周期中期(约 220 pg/mL)和黄体晚期/卵泡早期(约 310 pg/mL),最低水平在卵泡中期(约 125 pg/mL)和黄体中期(约 120 pg/mL))。
在黄体中期至晚期,激活素 A 水平逐渐升高(约 2.5 倍;P < 0.05),而抑制素 A、雌二醇和黄体酮均逐渐降低(约 10 倍;P < 0.001)"
---Changes in peripheral serum levels of total activin A during the human menstrual cycle and pregnancy - PubMed
“In females, FSH initiates follicular growth, specifically affecting granulosa cells.
With the concomitant rise in inhibin B, FSH levels then decline in the late follicular phase. This seems to be critical in selecting only the most advanced follicle to proceed to ovulation.
At the end of the luteal phase, there is a slight rise in FSH that seems to be of importance to start the next ovulatory cycle.”
---https://en.wikipedia.org/wiki/Follicle-stimulating_hormone
------分割线v.2.0------
到此为止我们对于月经周期内激素和组织变化相关的模型已经建立,接下来和大家讨论一个这个模型在临床实际中的应用,即古今中外,家喻户晓的--哺乳期避孕。
此处鸣谢泡泡是颗小肉丸同学,正是她之前关于哺乳期女性意外怀孕的提问和讨论将我的思路引向了此模型在这一临床情境中的应用。
先来说说基础知识:
催乳素通过抑制下丘脑分泌促性腺激素释放激素 (GnRH) 来防止排卵。 GnRH 的这种降低导致垂体前叶促黄体生成素 (LH) 和促卵泡激素 (FSH) 的分泌减少,从而阻止排卵。
通过临床试验和对孕妇产后体内的激素水平调查可发现:
- 分娩时,女性机体内催乳素水平仍然很高,而胎盘的分娩会导致孕酮、雌激素和人胎盘催乳素/HPL水平突然下降。 这种在催乳素水平高的情况下孕激素水平的大量下降会刺激乳房分泌原初乳。
- 当乳房受到刺激时,血液中的催乳素水平会上升,在大约 45 分钟内达到峰值,大约 3 小时后恢复到母乳喂养前的状态。
- 荷尔蒙内分泌控制系统在怀孕期间和出生后的最初几天推动乳汁分泌。 当乳汁供应更加稳固时,自分泌(或局部)控制系统开始。在这个阶段,从乳房中排出的乳汁越多,乳房产生的乳汁就越多。 研究还表明,更充分地排空乳房也会增加产奶率。
"Parents who bottle-feed, or do a combination of breastfeeding and bottle feeding, may get their periods as soon as five weeks after giving birth."
“During the first week after birth, prolactin levels in breastfeeding women fall about 50 percent. If a mother does not breastfeed, prolactin levels usually reach nonpregnant levels by seven days postpartum (Tyson et al., 1972).”
从临床实际以及相关研究可以得出以下结论:
- 分娩后哺乳期内泌乳活动与泌乳素水平并非呈高度对应关系
- 分娩后哺乳期内泌乳素水平与积极哺乳行为呈高度对应关系
从这个结论出发,哺乳期内泌乳素确实对血浆水平的FSH和LH 会产生抑制作用,从而导致FSH和LH水平无法维持卵泡正常生长发育的需求,卵泡周期暂时中止,所以没有排卵,也没有对应的月经现象发生。
但是分娩之后泌乳素的水平在没有积极哺乳活动的刺激下本身下降的极快,且泌乳素本身对于FSH和LH 的抑制作用也只存在较短的时效性(泌乳素呈脉冲式分泌,其他垂体前叶激素亦然),所以在一定时间以后(普遍统计结论为3个月到半年),女性机体内部卵泡周期其实已经回复了正常,故即使存在泌乳行为,但是仍然可以发生排卵活动。
由于泌乳素对于下丘脑的抑制作用,来自成熟卵泡的正向调节相对降低,血浆中FSH和LH水平对比正常月经周期中排卵时的峰值水平大幅下降,从而影响了黄体的成熟,导致黄体功能下降及黄体期的大幅缩短。因此女性机体内排卵后孕激素水平不足,子宫内膜未出现孕激素升高对应的增生,如若卵子未受孕,黄体期前后子宫内膜厚度较孕前女性相比相差较小,故而可能亦不能产生月经现象。(https://journals.sagepub.com/doi/pdf/10.1177/156482659601700412,page 4)
结合目前对于月经周期的模型,由于泌乳素对子宫和和卵巢不产生明显的直接影响,我们可以大胆猜测:产后女性子宫内膜厚度维持在经期前水平。结合相关文献结论--女性子宫在产后六周后即可恢复功能正常,且子宫内膜厚度已恢复到产前水平,符合前述推测。(OBGYN)
因此,在未施行积极哺乳的母亲中,哺乳期避孕的可靠性会大幅下降,即便女性月经未恢复正常,亦不代表女性机体此时不能受孕;因而,不建议因各种因素无法实施积极哺乳的妈妈们采取哺乳期避孕的方式。
如果希望采取积极哺乳行为而进行哺乳期避孕的话,目前学界的研究结论是:白天每4小时一次,夜晚每6小时一次,上不封顶;且相对而言只在产后六个月内(或到月经恢复截止)具有较好的效果。
---英文原稿如下---
Key Events in the Menstrual Cycle
There are four key events that comprise a typical menstrual cycle: follicular phase, ovulation, luteal phase and menstruation
* These events are distinguished by changes to hormonal levels, follicular development and the status of the endometrium
1. Follicular Phase
* Follicle stimulating hormone (FSH) is secreted from the anterior pituitary and stimulates growth of ovarian follicles
* The dominant follicle produces estrogen, which inhibits FSH secretion (negative feedback) to prevent other follicles growing
* Estrogen acts on the uterus to stimulate the thickening of the endometrial layer
2. Ovulation
* Midway through the cycle (~ day 12), estrogen stimulates the anterior pituitary to secrete hormones (positive feedback)
* This positive feedback results in a large surge of luteinizing hormone (LH) and a lesser surge of FSH
* LH causes the dominant follicle to rupture and release an egg (secondary oocyte) – this is called ovulation
3. Luteal Phase
* The ruptured follicle develops into a slowly degenerating corpus luteum
* The corpus luteum secretes high levels of progesterone, as well as lower levels of oestrogen
* Estrogen and progesterone act on the uterus to thicken the endometrial lining (in preparation for pregnancy)
* Estrogen and progesterone also inhibit secretion of FSH and LH, preventing any follicles from developing
4. Menstruation
* If fertilisation occurs, the developing embryo will implant in the endometrium and release hormones to sustain the corpus luteum
* If fertilisation doesn’t occur, the corpus luteum eventually degenerates (forming a corpus albicans after ~ 2 weeks)
* When the corpus luteum degenerates, estrogen and progesteron levels drop and the endometrium can no longer be maintained
* The endometrial layer is sloughed away and eliminated from the body as menstrual blood (i.e. a woman’s period)
* As estrogen and progesterone levels are too now low to inhibit the anterior pituitary, the cycle can now begin again
Estrogen suppresses FSH and LH secretion during the follicular phase through negative feedback inhibition of the hypothalamic-pituitary-ovarian axis.
Once plasma estrogen levels reach a critical threshold, and that level is maintained for at least 2 days(the period of matured follicle before its rupture), the negative feedback loop changes to a positive feedback loop and a surge in FSH and LH secretion occurs.
The menstral cycle related structures in the ovary can be subdivided into two group and three types:
* the follicle
* the corpus
* corpus luteum
* corpus albicans
To interpret the hormonal changes within the cycle, assume the growth of a follicle is spontaneous and is not regulated by the normal serum level of FSH and LH; only when a follicle reaches to its mature stage(late follicular phase), can it produce enough amount of estrogen and thus reach the level to produce a positive feedback on GnRH.
For the estrogen level is high in the serum and there is no corpus luteum in the ovary after ovulation, the progesterone level is low in the serum; thus the rise of FSH is not signnificant (negative feed back from estrigen), and the secretion of LH is stimulated as a result of elevated GnRh. This fluctuation mediates the preparation of a mature follicle to become a corpus luteum before ovulation.
After ovulation, the secretion of GnRH is no longer being stimulated for there is no mature follicle, the gradual decrease of LH and FSH mediate the maturation of corpus leuteum.
The growing corpus luteum produces a negative feedback on FSH and LH.
Without the stimulation of fertilization, corpus luteum atrophies to corpus albicans, leaving the FSH and LH level unregulated. For the new follicle is still growing after the first few days after menses, there is no new stimulation to GnRH, therefore the FSH and LH levels remain normal during the period when the old corpus luteum atrophies (corpus albicans) and the new follicle grows.
In females, FSH initiates follicular growth, specifically affecting [granulosa cells](https://en.wikipedia.org/wiki/Granulosa_cell "Granulosa cell").
With the concomitant rise in inhibin B, FSH levels then decline in the late follicular phase. This seems to be critical in selecting only the most advanced follicle to proceed to ovulation.
At the end of the [luteal phase](https://en.wikipedia.org/wiki/Luteal_phase "Luteal phase"), there is a slight rise in FSH that seems to be of importance to start the next ovulatory cycle.
During the menstrual cycle, mean serum activin A levels varied in a biphasic manner (by ANOVA, P = 0.02)
(with highest levels around midcycle (approximately 220 pg/mL) and the late luteal/early follicular phase (approximately 310 pg/mL) and nadirs in both midfollicular (approximately 125 pg/mL) and midluteal (approximately 120 pg/mL) phases).
Between the mid- to late luteal phase, the activin A level increased progressively (approximately 2.5-fold; P < 0.05), whereas inhibin A, estradiol, and progesterone all decreased progressively (approximately 10-fold; P < 0.001)
到这里文章基本上就结束了,后续如果鄙人在做题途中遇到了新的问题或者有了新的理解,我会及时和大家分享。
溯洄从之,道阻且右,且与诸君共勉!
此外本专栏名字和本文内容无关(狗头)
|
|





 发表于 2025-2-21 01:59:36
发表于 2025-2-21 01:59:36